Vulnerable Patients:
Secondary Immunodeficiency
RVIs can lead to prolonged ICU admissions and mechanical ventilation.3

Comorbidities: diabetes,4,5 GVHD,6 leukemia,4 lymphoma,4hematologic malignancies,6 metabolic disease4,5

Procedures: apheresis/ablation(CAR-T),7 inpatient/ outpatient surgery,5 hematologic transplant (HSCT/BMT),8solid organ transplant,6 anesthesia,4 splenectomy4

Treatment: chemotherapy,8 glucocorticoids,4,5immunosuppressants,4,5 immunotherapy and immunomodulatory agents4,5

Chronic and co-infection: COVID-19,9 HIV,4,5 viral hepatitis,10 influenza,10 pertussis,11 cytomegalovirus,4Epstein-Barr virus,4 herpes zoster,10 bacterial infection12

Malnutrition4,5

Environmental conditions: UV light,4,5 radiation5

Trauma: severe burns4,5
Patients requiring ventilation, intubation, or ICU admission3
Potential duration of ICU admission3
Failure to recognize and address these high-risk populations can result in long-term respiratory complications, increased hospitalizations, and mortality for patients.2,8
What next steps would you take for this patient?

Former smoker (1 pack/day for >25 years) with a history of COPD and emphysema
Received lung transplant and is receiving long-term immunosuppressants

Physical Exam
Presented to the ER with respiratory distress and severe confusion 3 months after receiving lung transplant
Physical examination results:

Hospital Course
Admitted to the ICU, with initiation of IV fluids and broad-spectrum antibiotics, and was placed on mechanical ventilation

On day 3, all cultures were NGTD except NP swab, which was positive for RSV.

Labs/Imaging
CT images show peribronchiolar nodular consolidations and ground glass opacifications
Significant laboratory values:- WBC: 3000 cells/μL
- Platelets: 85,000/μL
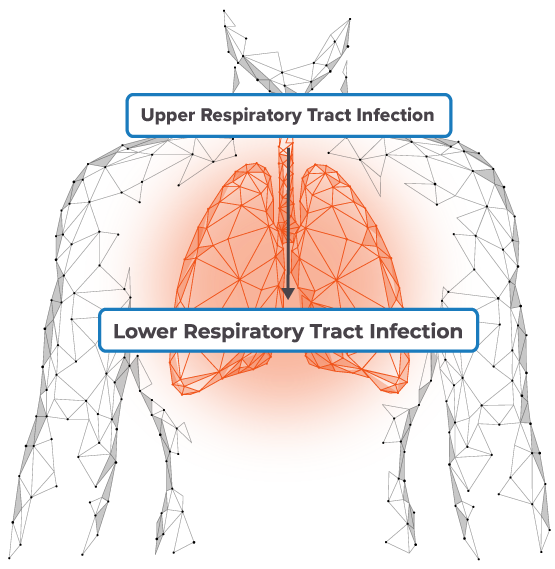
Immunocompromised patients face a number of clinical challenges associated with RVI, including co-infections, progression to lower respiratory tract infection, and potentially death.
Learn about the advantages and limitations of RVI management strategies in immunocompromised patients.
Cases are hypothetical. Images and descriptions are for illustrative purposes only
BMT, bone marrow transplant; COPD, chronic obstructive pulmonary disease; ER, emergency room; GVHD, graft-versus-host disease; HIV, human immunodeficiency virus; HSCT, hematopoietic stem cell transplant; ICU, intensive care unit; IV, intravenous; NGTD, no growth to date NP, nasopharyngeal; RSV, respiratory syncytial virus; RVI, respiratory viral infection; UV, ultraviolet; WBC, white blood cell.
References
1. Abbas S, et al. Int J Infect Dis. 2017;62:86-93. 2. Chatzis O, et al. BMC Infect Dis. 2018;18(1):111. 3. Schmidt H, et al. Influenza Other Respir Viruses. 2019;13(4):331-338. 4. Raje N, Dinakar C. Immunol Allergy Clin North Am. 2015;35(4):599-623. 5. Chinen J, Shearer WT. J Allergy Clin Immunol. 2010;125(2 Suppl 2):S195-S203. 6. Paulsen GC, Danziger-Isakov L. Clin Chest Med. 2017;38(4):707-726. 7. Buitrago J, et al. Clin J Oncol Nurs. 2019;23(2):42-48. 8. Hirsch HH, et al. Clin Infect Dis. 2013;56(2):258-266. 9. Shields AM, et al. J Allergy Clin Immunol. 2020; S0091-6749(20)32406-4. 10. Ruffner MA, et al. Front Immunol. 2017;8:665. 11. Solans L, Locht C. Front Immunol. 2019;9:3068. 12. Wiegers HMG, et al. BMC Infect Dis. 2019;19(1):938. 13. Cinetto F, et al. Eur Respir Rev. 2018;27(149):180019. 14. Baumann U, et al. Front Immunol. 2018;9:1837.